Nursing in Patients with Appendiksitis
1. Definition
Acute appendicitis is the most common cause of acute inflammation on the bottom right quadrant abdominal cavity, the most common cause for emergency abdominal surgery (Smeltzer, 2001).
Appendicitis is a condition in which the infection occurs in the appendix. In mild cases may recover without treatment, but many cases require laparotomy with removal of an infected appendix. If untreated, mortality is high, due to peritonitis and shock when an infected appendix destroyed. (Anonymous, Appendicitis, 2007)
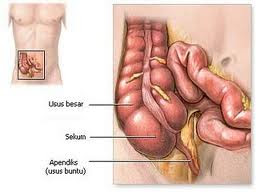
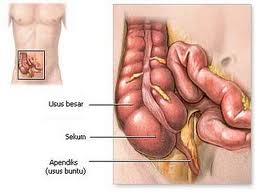
Appendicitis is the inflammation due to infection of the appendix or the appendix (appendix). These infections can lead to pernanahan. If the infection worsens, the appendix can rupture. The appendix is an intestinal tract clogged and prominent edges from the beginning of the colon or cecum (cecum). Appendix magnitude around the little finger and the hand is located in the lower right abdomen. The structure is like other parts of the intestine. However, the mucus glands that always contains a lot of mucus. (Anonymous, Appendicitis, 2007)
Appendicitis is an inflammation of the appendix / appendix (Anonymous, Appendicitis, 2007).
2. Classification
Classification appendicitis divided into 2 ie:
Acute appendicitis, divided into: acute appendicitis or segmentalis fokalis, ie after recovery will occur locally stricture. Appendicitis purulenta diffusion, which have accumulated pus.
Chronic appendicitis, divided into: chronic appendicitis fokalis or partially, after recovering stricture will occur locally. Chronic appendicitis appendix obliteritiva is tilted, usually found in old age.
3. Etiology
Appendiksitis is a bacterial infection caused by obstruction or blockage due to:
Hyperplasia of lymphoid follicles.
The presence fekalit in appendix lumen.
Tumor appendix.
The presence of foreign objects such as ascariasis worm.
Appendix mucosa erosion due to parasites such as E. Histilitica.
According to research, epidemiology shows eating foods low in fiber will cause constipation which can cause appendiksitis. This will increase the pressure of intra sekal, causing functional obstruction appendix and improve the growth of germs on the colonic flora.
4. Signs and symptoms
Quadrant abdominal pain is felt on the bottom and is usually accompanied by mild fever, nausea, vomiting and loss of appetite. Local tenderness at the point of Mc. Burney pressure when it's done. Pain press release may be encountered.
The degree of tenderness, muscle spasm, and if there is constipation or diarrhea does not depend on the severity of infection and location of the appendix. When the appendix circle behind the cecum, pain and tenderness can be felt in the lumbar region, when the tip is in the pelvis, these signs can only diketahuipada rectal examination. Pain at defecation shows that the end of the appendix close to the bladder or ureter. The presence kekeakuan on the bottom right of the rectum muscle may occur.
Tand Rovsing may arise by palpation of the left lower quadrant, which is paradoxical cause pain felt in the lower right quadrant. If the appendix has ruptured, the pain and can be more diffuse, abdominal distension and paralytic ileus due to clients condition worsened.
5. Pathophysiology
The main cause is obstuksi appendiksitis blockage which can be caused by hyperplasia of polikel lympoid is the most common cause of fekalit in lumen appendik.Adanya foreign objects such as: worms, stricture caused by inflammation, fibrosis karenan sebelunnya.Sebab another example: malignancy (carcinoid carcinoma).
Obsrtuksi appendix that causes mucus produced by mucous unstoppable, more and more mucus is unstoppable and suppress edema appendix wall and stimulate the tunica serosa and visceral peritoneum. Therefore, the neural appendix with the intestinal torakal X then the stimulus is perceived as pain around umblikus.
The collected mucus was then infected by the bacteria into pus, and then arise venous flow disturbance, while the artery is not interrupted, the inflammation that arises regarding peritomium parietal widespread and local, causing pain on the right below, this condition is called acute suppurative Appendisitis.
When the arterial flow is disrupted then arise allergens and is called by Appendisitis gangrenosa. When the wall acute appendix had burst, called Appendisitis perforation.
When the omentum adjacent bowel can surround the inflamed or perforated appendix will arise a local time, a condition called as Appendisitis abscess. In children - children as omentum is still short and thin, relatively long appendix, the appendix wall is much thinner and stamina is still lacking, as well as in older people because there's been blood vessel disorders, the perforation occurred more quickly. If these infiltrates Appendisitis cure the symptoms disappear and then arise in the future then there is chronic Appendisitis (Junaidi; 1982).
6. Complication
Perforation with abscess formation
Generalized peritonitis.
Pieloflebitis and liver abscesses, but rarely.
7. Prevention
Prevention of appendiksitis namely by lowering the risk obstuksi and inflammation of the appendix lumen. The pattern of elimination client should be assessed, because of obstruction by fekalit can occur because there is no strong diet and treatment of high serat.Perawatan worm also creates the risk of disease. Rapid introduction of the symptoms and signs appendiksitis reduce the risk of gangrene, perforation and peritonitis.
8. Management
In appendiksitis acute, the best treatment is surgery appendix. Within 48 hours must be done. Patients in obsevarsi, rest in the Fowler position, given antibiotics and are given food that does not stimulate persitaltik, if there is perforation given drain in the lower right abdomen.
Pre-operative action, including patients in hospital, given antibiotics and compress to lower the temperature of the patient, the patient was asked to tirabaring and fasted.
Operative action; appendiktomi.
Post-operative action, one day post-surgical clients are encouraged to sit up in bed for 2 x 30 minutes, the next day of soft food and standing outside the room, the seventh day wound stitches removed, the client's home.
A. Assessment
Patient Identity
The identity of the client's name, age, sex, marital status, religion, tribe / nation, education, occupation, income, address and registration number.
Nursing History
Medical History now: complaints of pain in postoperative wound apendektomi, nausea, vomiting, increased body temperature, increased leukocytes.
Past Medical History
Physical examination
Cardiovascular System: To determine vital signs, presence or absence of jugular vein distension, pale, edema, and abnormal heart sounds.
Hematological system: To determine whether there is an increase in leukocytes is a sign of infection and bleeding, nosebleeds splenomegaly.
Urogenital system: There is absence of tension of the bladder and back pain complaints.
Musculoskeletal System: To determine whether there is difficulty in movement, pain in bones, joints and there are fractures or not.
The immune system: To determine whether there is lymph node enlargement.
Examination Support
Routine blood tests: to determine an increase in leukocytes is a sign of infection.
Abdominal x-ray examination: to know the existence of post-surgical complications.
Appears Possible Nursing Diagnosis
Pain associated with incision wounds to the right lower quadrant abdominal postoperative appenditomi.
Activity intolerance related to restriction of motion secondary to pain.
High risk of infection associated with invasive procedures appendiktomi.
The risk of lack of fluid volume in relation to the restriction of oral fluid intake.
Intervention
Nursing Diagnosis 1. :
Pain associated with incision wounds on postoperative abdominal mesial area appendiktomi
Goal
Pain is reduced / lost with
Criteria Results:
Seemed relaxed and could sleep properly.
Intervention
Assess the scale of pain location, pain characteristics and report changes accordingly.
Maintain a break with the semi powler.
Encourage early ambulation.
Give your entertainment activities.
Kolborasi team of doctors in the provision of analgesics.
Rational
Useful in surveillance and keefesien medicine, healing progress, changes and characteristics of pain.
Eliminating stress is increased by abdominal supine position.
Improve kormolisasi organ function.
increase relaxation.
Pain relief.
Nursing Diagnosis 2. :
Activity intolerance related to restriction of motion secondary to pain
Goal
Tolerance activity
Criteria Results:
Clients can move without restriction
Careful not to move.
Intervention
note the emotional response to the mobility.
Provide activities in accordance with state clients.
Give the client to passive motion exercises and active movements.
Assist clients in conducting activities that are burdensome.
Rational
Forced immobilization will increase anxiety.
Increasing organ kormolitas sesuiai expected.
Improving body mechanics.
Avoiding things that can aggravate the situation.
Nursing Diagnosis 3. :
High risk of infection associated with invasive procedures appendiktomi
Goal
Infection does not occur
Criteria Results:
There were no signs of infection and inflammation
Intervention
Measure vital signs
Observation of signs of infection
Perform wound care using aseptic technique and septic
Observation of the incision wound
Rational
To detect early symptoms of the onset of the infection
Early detection of infection will be easily
Lowering the risk of infection and spread of bacteria.
Provide early detection of infection and the development of sores.
Nursing Diagnosis 4. :
The risk of lack of fluid volume restriction pemasuka n berhubungna with oral fluid
Goal
Lack of volume of liquid does not occur
Intervention
Measure and record intake and output of body fluids
Monitor vital signs: Evaluation of pulse, capillary filling, skin turgor and mucous membranes
Collaboration with the team physician for the administration of intravenous fluids
Rational
Accurate documentation will help in identifying the discharge or replacement needs.
Indicators of circulating fluid volume and hydration needs intervention
Maintain circulating volume when oral intake is not sufficient and improve kidney function
Bibliography
Barbara Engram, Askep Medical Surgery, Volume 2, EGC, Jakarta.
Carpenito, Linda Sell, Nursing Diagnosis, Issue 8, EGC, 2000, Jakarta.
Doenges, Marlynn, E, Plan Nursing, Edition III, EGC, 2000, Jakarta.
Elizabeth, J, Corwin, monks Fatofisiologi pocket, EGC, Jakarta.
Esther, Monica, SKP, Medical Surgical Nursing (Gastrointestinal Approach), EGC, Jakarta.
Peter, M, Nowschhenson, Practical Aspects of Surgery for Beginners. Script Development Jakarta
0 Response to "Nursing in Patients with Appendiksitis"
Posting Komentar